



Coxarthrosis - a cartilaginous disease of the pelvis and thigh
Diagnosis of coxarthrosis at the National Center of Surgery
We would like to remind you that Beka Ghambashidze, a traumatologist and orthopedic surgeon, offers a free consultation at our clinic. During this consultation, the patient will receive highly skilled services for diagnosis and treatment that take into account current treatment principles and protocols. For more details, click the promotion: Promotion of a traumatologist.
You will learn about the pathology that prevents the patient from freely moving and causes them to lose their active lifestyle rhythm. An expert on this condition and its treatments, Beka Ghambashidze is a board-certified orthopedic-traumatologist with the National Center of Surgery and has attended AO seminars and master classes. He presents his experience and knowledge abroad :
-What is coxarthrosis?
-It is a degenerative alteration of the cartilaginous surface of the pelvic-femoral joint with additional deformation of the articular surface, which lowers the patient's quality of life and produces discomfort, gradual movement restriction, and stiffness.
-How prevalent is the condition and in what types of patients does it occur?
-This devastating illness is common in Georgians, particularly among women. It comes in a variety of forms and stages that vary from one another in their underlying causes and can therefore be found in all age groups. Diagnosis of the disease in Georgia is mostly found in the population of retirement age, however, it is not unusual for young and postmenopausal women to be diagnosed with the condition in Georgia. This is because the bone tissue is notably deficient following the menopause, and the degree of osteoporosis reaches a high level. Pathology is still mostly formed as a result of local blood circulation imbalance.
-On what basis is coxarthrosis mainly manifested in females?
-There is a theory that the female sex's pelvic anatomy would be to responsible for this. Since women's pelvises are anatomically wider than men's, there is a bigger angle at the pelvic-femoral joint than at the knee, which in turn provokes incorrect loading of the joint and wear of the articular cartilage. Additionally, it is thought that inadequate blood flow to women's pelvic joints, which results in tissue hypoxia, could be a contributing factor. When the joint can't get the nutrients it needs, cartilage tissue starts to deteriorate.
-Dysplasia: What is it? What does it have to do with coxarthrosis, and what indications might it present clinically?
- A medical disorder called Pelvic-femoral joint dysplasia disturbs the alignment of the femoral head and the acetabulum/femur socket. The condition is clinically characterized by pain and movement restriction in the pelvic-femoral joint region, as well as shortening of the limb, a positive symptom of Barlow and Ortolani (when bending and lifting the limbs, the fall is corrected and a squeaking sound is heard), and in the later stages, lameness.
The acetabulum/femur socket is inconsistent, the femoral head centers are off, and the femoral neck-shaft angle is increasing against the backdrop of dysplasia. The disturbance of joint biomechanics (uneven load distribution) and alteration in the joint's center of rotation caused by these changes hasten the development of coxarthrosis and deepens the dystrophic process.
-What are the complaints of this disease?
-The primary concerns of patients are pain and restricted joint motion, which worsens and eventually results in lameness.
-How is coxarthrosis diagnosed? What is the initial sign?
-Pain is the primary symptom, as was already mentioned. In the beginning, the patient only experiences discomfort after exerting themselves physically, the pain goes away when the patient is at rest, thus the patient is unaware of the severity of the issue. A correct and prompt alternative diagnosis is crucial because spinal diseases might potentially be the cause of pain (particularly if it is not followed by lameness). It is crucial that the patient seeks out a specialist as soon as possible.
-How do you conduct research on the joint to obtain a diagnosis? What details does it reveal?
-While physical examination, radiographs, and Ultrasound are used to make diagnoses in children, computed tomography or magnetic resonance imaging is crucial in making diagnoses in adults.

-Which diseases of the spine can cause coxarthrosis and why?
-The anatomical axis of the musculoskeletal system is breached, and the patient's stride changes in accordance with the curvature of the spine, which can be the reason of this. The pelvic-femoral joint, which is on the pathology's side, is particularly pressured, which along with time results in deterioration. Coxarthrosis may, on the other hand, aid in the development of spinal diseases.
-What negative effects might an escalating diagnosis have?
-Disabilities might result from limb and pelvic joint disorders. Other large joints are also dynamically damaged by this illness, which alone suggests a severe decline in the patient's quality of life.
-What type of coxarthrosis is present, if any?
-It can be inherited or acquired.
Congenital pathology is the result of incomplete development of joint components during pregnancy - the so-called, Dysplastic coxarthrosis.
Acquired or secondary disease can be brought on by a number of factors, which are based on disruption of blood flow in the pelvic-femoral joint, local inflammation, and, as a result, depletion of cartilage tissue.
According to the stage of the degenerative-dystrophic process, coxarthrosis is classified into 4 degrees based on clinical symptoms and X-ray alterations. Three varieties of dysplasia exist:
- Mild dysplasia;
- Moderate to marked dysplasia;
- Severe dysplasia to carcinoma in situ.
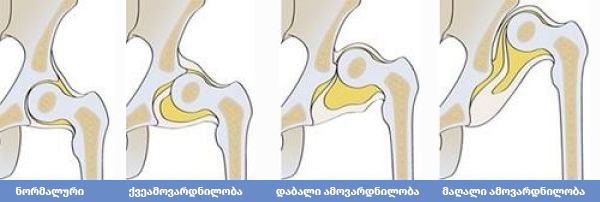
The femur's relation to the acetabulum/femur socket is where they diverge from one another.
-In the case of a congenital disease, does a parent's misbehavior during pregnancy cause it to have any genetic or other cause?
-The presence of the fetus in the pelvis, during which the fetus's pelvic-femoral joints are loaded wrongly due to the fetus's location, affects the frequency of congenital dysplastic coxarthrosis. This leads to an imperfect interaction between the femoral head and the acetabulum/femur socket. This is crucial in the final trimester of pregnancy when the fetus grows and, in reality, removal of the femoral head and the acetabulum/femur socket is required for space reasons. The development of dysplasia is also significantly influenced by the feminine gender, genetic susceptibility, early pregnancy, and dehydration.
-How do you treat coxarthrosis and what manipulations are performed during the operation?
-Depending on the disease's stage, treatment options include surgery and conservative measures. Disease is emphasized that medication can only be used to temporarily reduce discomfort and halt the growth of coxarthrosis, not to cure it. The only effective treatment for this illness and the issues it causes is surgery.
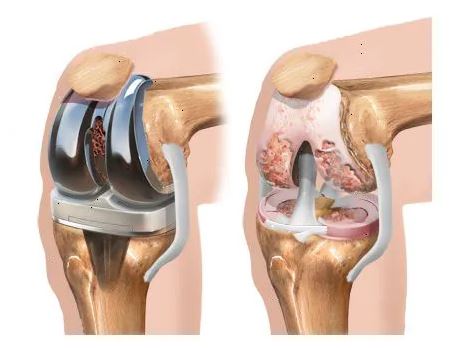
The injured femur's head is removed during open Endoprosthesis, and the acetabulum/femur socket is treated and replaced with artificial, metal parts that will take the role of these anatomical pieces for the patients. We utilize cement prostheses, which we put the metal in close touch with the bone, when the patient is very young and their bone stores are intact. We also employ cement prostheses when the patient is relatively old or has osteogenesis (we utilize medical cement to fix the prosthetic components since the bone resource in the patient is in poor condition.) In my practice, endoprostheses are necessary for patients as young as 17 and as old as 103. Each patient's prosthesis is selected specifically for them. The ideal size of the femur and femur socket component, the degree of femoral neck resection, and the length of the endoprosthesis neck can all be determined through preoperative X-ray examination.
-What is the greatest operational challenge?
- Obviously, endoprosthesis is defined by all the challenges that come with any other procedure, but getting the prosthesis in contact with the living bone is what matters most. The prosthesis's durability later on depends on how well the bone canal has been prepared for adaption to it. For this reason, prostheses with rough surfaces were developed, which facilitates the insertion of the bone.
-What are the treatment options before surgery is required? What kind of activities is the patient supposed to do?
-Prior to surgery, we turn to conservative treatment, which, as previously indicated, provides momentary pain relief. Both medicine and physical therapy can help with this. Swimming is advised as an activity to build up the muscles, but ultimately, surgery is still required.
-Is there a current approach or procedure for treating coxarthrosis?
-Pelvic-femoral endoprosthesis - which replaces joint components with synthetic counterparts, is currently the „gold standard” of treatment. My professor Professor Tornike Nozadze, whose legacy we are happy to carry on with the next generation of doctors, introduced this procedure to Georgia in 1995. After a successful surgical procedure and appropriate rehabilitation, the patient no longer experiences discomfort or movement restrictions and resumes their regular routine.
-What kind of lifestyle should someone lead to prevent the onset of this disease? Can we classify it as an occupational illness?
- Coxarthrosis can occur in any job, but it is more common in those that require physical effort and prolonged standing owing to activities. Only leading a healthy lifestyle, managing body mass index, and promptly seeing a doctor in the event of problems will avoid coxarthrosis!
-What connection exists between coxarthrosis and obesity? Can it be regarded as one of the causes of the disease's onset?
-The pathogenesis of coxarthrosis is heavily influenced by weight. Obese people face a variety of metabolic diseases in addition to joint strain, which accelerate the progression of the disease at the level of their metabolic rate. In order to avoid premature metal wear and frequent surgical intervention after endoprosthesis and to prevent coxarthrosis, weight control is crucial.
The National Center of Surgery works 24/7, every day!
Wish you health!
What are patients interested in
Coxarthrosis, oatmeal
Qauestion:: Hello, I was diagnosed with onset of coxarthrosis and take plexus. I’d like to know if daily consumption of oatmeal is recommended, they say oatmeal causes bone erosion.
Pelvic-femoral joint endoprosthesis
Qauestion:: Welcome, early in November, the wife had pelvic thigh endoprosthesis. Golden staphylococcus was discovered after a dental implant was placed, and National Tuberculosis Center (Reference Laboratory) has been managing the TB treatment for more than a year. Following surgery, the condition dramatically improved for the first two months before deteriorating. Although the X-ray revealed no problems, the leg pain is worse. It has a slight swallowing and originates mostly in pelvis. Did you offer any suggestions. Thank you in advance.
Toe pain
Qauestion:: I have pain in the right long toe/following the big toe/ already for two months. I’m already limping. Initially, I had a pain in pads of feet, then in the toe as well. Toe is a bit swollen. It burns and aches as if I was doused with hot water. If you can’t help, who should I contact. Is it dangerous?






